Reticulocyte Count
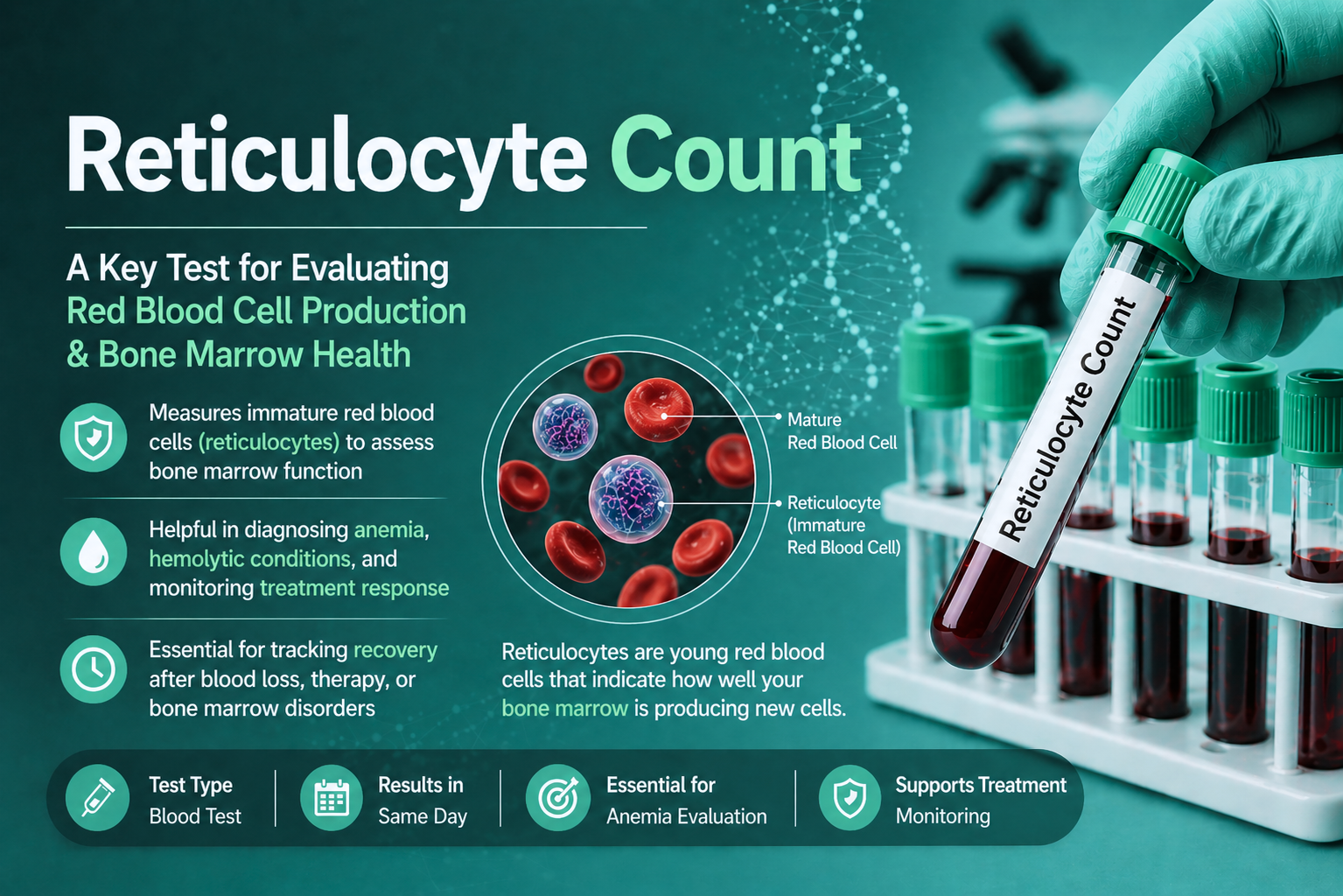
Table of Contents
Definition
A reticulocyte is an immature, anucleated red blood cell (RBC) that represents the penultimate stage of erythropoiesis. After the orthochromatic erythroblast extrudes its nucleus in the bone marrow, it becomes a reticulocyte.
These cells remain in the marrow for about 2–3 days and then circulate in the peripheral blood for 1 day before maturing into a functional erythrocyte. Their defining characteristic is the presence of residual ribosomal RNA (rRNA), which can be visualized using specific laboratory techniques.
Clinical Significance
In the diagnostic laboratory, the reticulocyte count is more than just a number; it is a dynamic indicator of bone marrow activity. While the RBC count tells you the current “inventory” of red cells, the reticulocyte count tells you the “production rate.”
Here is the detailed clinical significance of this parameter for medical professionals:
1. Classification of Anemias (Pathophysiological Approach)
The most critical use of the reticulocyte count is to differentiate between the two main categories of anemia. This helps the clinician decide whether to look for a “source” problem (bone marrow) or a “loss” problem (peripheral).
A. Hyperproliferative Anemia (High Reticulocyte Count)
An elevated count (> 2.5%) indicates that the bone marrow is healthy and is working overtime to compensate for a decrease in red blood cells.
Hemolytic Anemias: Whether due to sickle cell disease, G6PD deficiency, or autoimmune factors, the premature destruction of RBCs triggers the marrow to release reticulocytes early.
Acute Hemorrhage: Following a major bleed, the body’s natural erythropoietin levels spike, leading to a “reticulocyte response” within 3–5 days.
Post-Therapeutic Response: A sudden rise in reticulocytes is the first sign that treatment for nutritional anemias (Iron, B12, or Folate) is working.
B. Hypoproleferative Anemia (Low Reticulocyte Count)
A low or “normal” count in the presence of anemia is actually abnormal. It suggests the bone marrow is not responding to the body’s needs.
Nutritional Deficiencies: In early stages of iron or B12 deficiency, the “building blocks” for new cells are missing.
Bone Marrow Failure: Conditions like Aplastic Anemia or leukemia crowd out the erythroid precursors.
Chronic Kidney Disease (CKD): Reduced production of Erythropoietin (EPO) by the kidneys leads to low reticulocyte production.
2. Monitoring Therapeutic Efficacy
The reticulocyte count is a “leading indicator,” whereas Hemoglobin and Hematocrit are “lagging indicators.”
Iron Deficiency: After starting oral iron, the reticulocyte count begins to rise in 3–5 days and peaks around 7–10 days. The Hemoglobin may not show a significant increase for 2–3 weeks.
Erythropoietin Therapy: For patients on dialysis or chemotherapy, the reticulocyte count is used to monitor the dosage and effectiveness of EPO injections.
3. Assessment of Bone Marrow Transplant
Following a bone marrow or stem cell transplant, the Immature Reticulocyte Fraction (IRF)—a parameter provided by automated analyzers—is the earliest sign of “engraftment.” When the new marrow begins to function, reticulocytes appear in the blood even before the total WBC or platelet counts begin to rise.
4. Distinguishing “Acute” vs. “Chronic” Conditions
Acute Blood Loss: Shows a significant reticulocytosis.
Chronic Blood Loss (like a slow GI bleed): Often leads to iron deficiency over time, resulting in a low or normal reticulocyte count because the marrow eventually runs out of iron to keep up production.
5. Identifying “Shift” Reticulocytes
In severe anemia, the hormone erythropoietin doesn’t just increase production; it causes the marrow to release reticulocytes prematurely. These are called “stress” or “shift” reticulocytes.
Laboratory Observation: These cells are larger, contain more RNA (heavier reticulum), and appear more “blue” (polychromasia) on a standard blood film.
Clinical Calculation: This is why the Reticulocyte Production Index (RPI) is mandatory. Without calculating the RPI, a lab technologist might over-estimate how well the marrow is actually performing.
Summary Table for Lab Reports
| Condition | Reticulocyte Count | Clinical Interpretation |
| Untreated Iron Deficiency | Low / Normal | Production Failure (Marrow lacks raw materials) |
| Sickle Cell Crisis | Very High | Compensation for Hemolysis |
| Aplastic Anemia | Extremely Low | Marrow Failure (Aplasia) |
| Pregnancy | Slightly High | Normal physiological response to increased blood volume |
| High Altitude | High | Physiological response to hypoxia |
Methods & Principle
As a laboratory professional, you know that while automation is the standard, the manual method remains the “gold standard” for troubleshooting and validation.
The underlying principle differs strictly between manual and automated platforms.
Manual Method: Supravital Staining
Principle: Reticulocytes are living cells that lack a nucleus but contain residual Ribosomal RNA (rRNA). Because these cells are not fixed, they are stained in a “supravital” state.
Reaction: Basic dyes (New Methylene Blue or Brilliant Cresyl Blue) penetrate the cell and react with the acidic rRNA. This causes the RNA to precipitate, forming a dark blue, filamentous network or “reticulum.”
Reference Definition: According to the ICSH, a cell is classified as a reticulocyte if it contains two or more granules of blue-stained material that are not attached to the cell membrane.
Automated Method: Flow Cytometry
Principle: Uses fluorescent dyes (e.g., Thiazole Orange, Polymethine, or Auramine O) that bind specifically to nucleic acids.
Detection: As cells pass through a laser, the analyzer measures the intensity of the Fluorescence and Forward/Side Light Scatter.
Significance: Higher fluorescence indicates a higher concentration of RNA, identifying the “youngest” reticulocytes (Immature Reticulocyte Fraction – IRF).
2. Standard Manual Methodology (WHO/ICSH Protocol)
To ensure precision, the following standardized steps are required:
Anticoagulant: K₂EDTA or K₃EDTA blood (must be processed within 4 hours at room temperature or 24 hours if refrigerated at 4°C).
Mixing: Mix equal volumes (usually 2–3 drops) of filtered stain and whole blood in a 10 x 75 mm tube.
Incubation: Incubate at room temperature for 10 to 15 minutes.
Spread: Resuspend the cells gently and prepare thin “wedge” smears.
Counting (The Miller Ocular): To reduce the statistical error of small numbers, use a Miller Graticule.
Count reticulocytes in the large square (Square A).
Count total RBCs in the small square (Square B).
3. Clinical Significance & Reference Ranges
The clinical utility is primarily focused on Erythropoietic activity.
Reference Ranges (Henry’s 22nd Edition)
| Age Group | Range (%) | Absolute Count (103/μL) |
| Newborns (0–7 days) | 1.8 – 4.6% | 70.2 – 252.8 |
| Adults | 0.5 – 1.5% | 20.0 – 80.0 |
Diagnostic Interpretations
Regenerative Anemia (High Count): * Hemolytic Anemias: Hereditary Spherocytosis, G6PD deficiency, or Autoimmune Hemolysis.
Blood Loss: Acute hemorrhage (peaks at 7–10 days).
Non-Regenerative Anemia (Low Count):
Marrow Failure: Aplastic anemia, bone marrow infiltration (leukemia).
Nutritional Deficiency: Untreated Iron, B12, or Folate deficiency.
EPO Deficiency: Secondary to Chronic Kidney Disease.
4. Advanced Clinical Indices (Reference Only)
In modern diagnostics, two parameters are superior to the raw percentage:
Reticulocyte Production Index (RPI): Corrects for both the patient’s anemia and the “shift” (premature release) of reticulocytes.
Calculation: RPI = Observed Retic % x {Patient Hct / 45} / Maturation Factor
Interpretation: RPI > 3 indicates a robust response; RPI < 2 indicates an inadequate response
Immature Reticulocyte Fraction (IRF): The most sensitive marker for Bone Marrow Engraftment post-transplant or the earliest response to iron therapy.
5. Potential Interferences (Sources of Error)
False Highs: Pappenheimer bodies (iron granules), Heinz bodies (denatured Hb), Howell-Jolly bodies (DNA remnants), or heavy Malarial stippling.
False Lows: Under-incubation, high glucose levels (inhibits staining), or using old/clotted samples.
Specimen Requirements
1. Primary Sample Type
Whole Blood: The specimen must be whole blood to ensure the reticulocytes remain in their natural suspension for counting.
Anticoagulant: K₂EDTA (Dipotassium Ethylenediaminetetraacetic acid) or K₃EDTA is the gold standard.
Mechanism: EDTA preserves the morphology of red blood cells and prevents platelet clumping, which is critical because automated analyzers may misidentify small platelet clumps as reticulocytes.
Note: Avoid Heparin as it can cause a blue background tint on the slide, interfering with manual microscopic interpretation.
2. Collection Volume
Adults: A standard 3.0 mL to 5.0 mL “Lavender Top” tube.
Pediatrics/Neonates: 250 μL to 500 μL in a micro-collection EDTA container (bullet).
Minimum Volume: For manual counts, as little as 50 μL (approx. 2 drops) of blood is required, but automated analyzers typically need a minimum “dead volume” of 200–500 μL depending on the instrument model.
3. Stability and Storage
The timing of the test is critical because RNA degrades over time, leading to falsely decreased counts.
Room Temperature (18–25°C): Stable for up to 6 to 8 hours. Testing should ideally be performed as soon as possible.
Refrigerated (2–8°C): Stable for up to 24 to 48 hours. If a sample cannot be processed immediately, refrigeration is mandatory to slow down the maturation of reticulocytes into mature erythrocytes.
Warning: Samples older than 48 hours should be rejected or reported with a disclaimer, as the RNA reticulum will disappear, resulting in a false-negative result.
Criteria for Specimen Rejection (Quality Control)
To maintain the E-E-A-T (Expertise, Authoritativeness, Trustworthiness) of your laboratory:
| Reason for Rejection | Impact on Result |
| Clotted Sample | Falsely decreased count; cells are trapped in the fibrin clot. |
| Hemolyzed Sample | Inaccurate count; RBC fragments may be miscounted as reticulocytes. |
| Incorrect Tube (e.g., Citrate/Heparin) | Morphological changes and staining interference. |
| Insufficient Volume (Underfilled) | Excess EDTA causes RBC shrinkage (crenation), affecting automated light scatter. |
| Old Samples (>48 hrs) | Falsely low results due to RNA degradation. |
Pre-Analytical Considerations
Fasting: Not required.
Mixing: The tube must be inverted gently 8–10 times immediately after collection to ensure proper anticoagulation. Before testing in the lab, the sample should be placed on a mechanical mixer for at least 5 minutes.
Capillary vs. Venous: Venous blood is preferred. However, capillary blood (heel prick/finger stick) is acceptable for neonates provided the flow is free (no “milking” the site, which introduces tissue fluid and causes clotting).
Clinical Pro-Tip for MedLabify Readers
When performing a manual count on a severely anemic patient, the blood-to-stain ratio should be adjusted. Instead of a 1:1 ratio, use 2 drops of blood to 1 drop of stain to increase the density of cells on the slide, making it easier to find 1,000 RBCs to count.
Reference Ranges & Clinical Interpretations
1. Reference Ranges
Reference ranges for reticulocytes must be interpreted based on age, as neonates have significantly higher erythropoietic activity.
A. Relative Reticulocyte Count (Percentage)
This is the number of reticulocytes per 100 RBCs.
Adults: 0.5% – 1.5% (some labs cite up to 2.5% depending on methodology).
Newborns (Full-term): 2.0% – 6.0% (falls to adult levels within 1–2 weeks).
Infants: 1.0% – 3.0%.
B. Absolute Reticulocyte Count (ARC)
The ARC is considered more clinically accurate than the percentage because it is not influenced by the total RBC count.
Formula: ARC = {Retic % x RBC Count (10¹²/L)} / 100
Adult Reference Range: 20 x 10^9/L to 120 x 10^9/L (or 20,000–120,000/µL).
2. Clinical Interpretations: The “Why”
The reticulocyte count is the primary tool used to determine if an anemia is Regenerative (marrow is responding) or Non-Regenerative (marrow is failing).
A. Reticulocytosis (Increased Count)
A high count indicates an appropriately responding bone marrow.
Hemolytic Anemias: The most common cause. Rapid destruction of RBCs (e.g., Sickle Cell, G6PD deficiency, or Malaria) triggers a massive release of young cells.
Post-Hemorrhage: After acute blood loss, the count begins to rise in 24–48 hours, peaking at 7–10 days.
Response to Therapy: A “reticulocyte crisis” (a sharp rise) is seen after treating Iron, B12, or Folate deficiencies. This is a positive sign that the treatment is effective.
Physiological Stress: Pregnancy and high-altitude living naturally increase erythropoietin levels, leading to higher reticulocyte counts.
B. Reticulocytopenia (Decreased Count)
A low count in the presence of anemia is a “critical” finding, suggesting a production defect.
Aplastic Anemia: Global bone marrow failure where the “factory” stops producing all cell lines.
Nutritional Deficiencies: In untreated iron or megaloblastic (B12/Folate) anemia, the marrow lacks the raw materials to build cells.
Chronic Kidney Disease (CKD): The kidneys fail to produce Erythropoietin (EPO), so the marrow never receives the signal to produce RBCs.
Bone Marrow Infiltration: Leukemia, lymphoma, or metastatic cancer “crowds out” normal erythroid precursors.
Infections: Certain viruses, like Parvovirus B19, specifically target and destroy erythroid progenitor cells.
3. Correcting for Anemia: The Logic Core
In anemic patients, a “normal” reticulocyte percentage (e.g., 1.0%) is actually dangerously low. You must use corrected indices to provide a true clinical picture.
Corrected Reticulocyte Count (CRC)
The CRC adjusts the percentage to account for the reduced number of total RBCs in anemic patients.
Reticulocyte Production Index (RPI)
This is the “Gold Standard” for interpretation. It corrects for the “Shift”—the fact that in severe anemia, the marrow releases reticulocytes prematurely, and they stay in the blood for 2.5 days instead of 1 day.
Interpretation of RPI:
RPI > 3: Excellent marrow response (Hemolysis or Blood loss).
RPI < 2: Inadequate response (Hypoproliferative anemia or production failure).
4. Summary for Diagnostic Reporting
| Finding | RPI Value | Possible Diagnosis |
| High Retic + High RPI | > 3 | Hemolytic Anemia, Acute Hemorrhage. |
| High Retic + Low RPI | < 2 | Ineffective Erythropoiesis (e.g., Thalassemia). |
| Low Retic + Low RPI | < 2 | Aplastic Anemia, Iron Deficiency, CKD. |
Quick Stats
| Feature | Details | Critical Lab Insights |
| Test Type | Hematology / Erythropoietic Marker | A definitive indicator of bone marrow regenerative capacity. It distinguishes between marrow failure and peripheral RBC destruction. |
| Sample Type | Whole Blood (EDTA) | K2 or K3 EDTA (Lavender Top). Heparin is contraindicated as it creates a blue background haze on manual smears, obscuring the reticulum. |
| Stain Method | Supravital Staining | Uses New Methylene Blue or Brilliant Cresyl Blue. Staining must occur while cells are “alive” (unfixed) to precipitate residual ribosomal RNA. |
| Primary Metric | Percentage (%) or Absolute Count | Absolute Reticulocyte Count (ARC) is clinically superior to percentage as it isn’t “falsely” inflated by low total RBC levels in anemic patients. |
| Fasting Required? | No | Non-fasting. However, extremely lipemic samples can interfere with automated optical scatter or fluorescence-based counting channels. |
| Standardization | ICSH / Miller Ocular | Manual counts are standardized using a Miller Graticule to minimize distribution errors. Automated methods are standardized via fluorescent RNA-binding dyes. |
| Turnaround Time | 20–40 Minutes | Includes 10–15 mins incubation for manual methods. Often ordered as part of an anemia workup following an abnormal CBC result. |
| Biological Half-life | ~24 Hours | Reticulocytes circulate for roughly 1 day in peripheral blood before losing their RNA and maturing into functional erythrocytes. |
| Normal Range | 0.5% – 1.5% (Adults) | Range is significantly higher in neonates (2%–6%). Normalization to adult levels typically occurs within the first 1–2 weeks of life. |
| RPI Cut-off | > 3.0 (Adequate) | An RPI < 2.0 in an anemic patient indicates an inadequate marrow response (Hypoproliferative), necessitating further investigation into production defects. |
| Key Limitation | Inclusion Interference | Manual counts can be falsely elevated by Pappenheimer bodies, Heinz bodies, or Howell-Jolly bodies, which may be mistaken for reticulum. |
FAQs
Q1: Why can’t I use a Wright-Giemsa stain to count reticulocytes? A: Reticulocytes require supravital staining. Wright-Giemsa stain involves methanol fixation, which kills the cell instantly and prevents the RNA from precipitating into a visible reticulum. On a standard Wright-stained smear, you may see polychromasia (bluish-gray cells), which is a subjective indicator, but you cannot perform a quantitative count.
Q2: What is the clinical significance of the Immature Reticulocyte Fraction (IRF)? A: IRF is an automated parameter that measures the “youngest” reticulocytes (those with the highest RNA content). It is the earliest indicator of bone marrow engraftment post-transplant or recovery from chemotherapy—often rising days before the absolute reticulocyte count or total WBC count increases.
Q3: How do I distinguish a reticulocyte from a Heinz body under the microscope? A: Both appear blue with supravital stains, but their morphology differs:
Reticulocytes: Contain a network or at least two dots of deep blue material located within the cytoplasm.
Heinz Bodies: Usually appear as round, rigid inclusions attached to the inner membrane of the RBC. They represent denatured hemoglobin (common in G6PD deficiency).
Q4: Why must I calculate the RPI if the Reticulocyte Percentage is already high? A: A high percentage can be deceptive. In severe anemia, the “total RBC pool” is small, making even a few reticulocytes look like a high percentage. Additionally, the marrow releases these cells prematurely (shift cells), so they stay in circulation longer. The Reticulocyte Production Index (RPI) “penalizes” the count for these factors to show the real daily production rate.
Q5: Can a reticulocyte count be used to monitor chronic kidney disease (CKD)? A: Yes. Since the kidneys produce Erythropoietin (EPO), patients with CKD often have a low reticulocyte count (reticulocytopenia) because the signal to produce RBCs is missing. It is used to monitor the effectiveness of recombinant EPO therapy.
Q6: Does a high reticulocyte count always mean the patient is improving? A: Not necessarily. If the patient has hemolytic anemia, the count is high because cells are being destroyed as fast as they are being made. It indicates the marrow is trying to help, but it doesn’t mean the anemia is resolved. However, in a patient being treated for iron deficiency, a high count is a confirmed sign of recovery.
Q7: What is “Reticulocyte Crisis”? A: This is a laboratory term for the rapid, massive increase in reticulocytes (often peaking at 10–20%) seen approximately 5 to 10 days after successful treatment of a nutritional anemia (like Vitamin B12 or Iron deficiency).