Bleeding Time
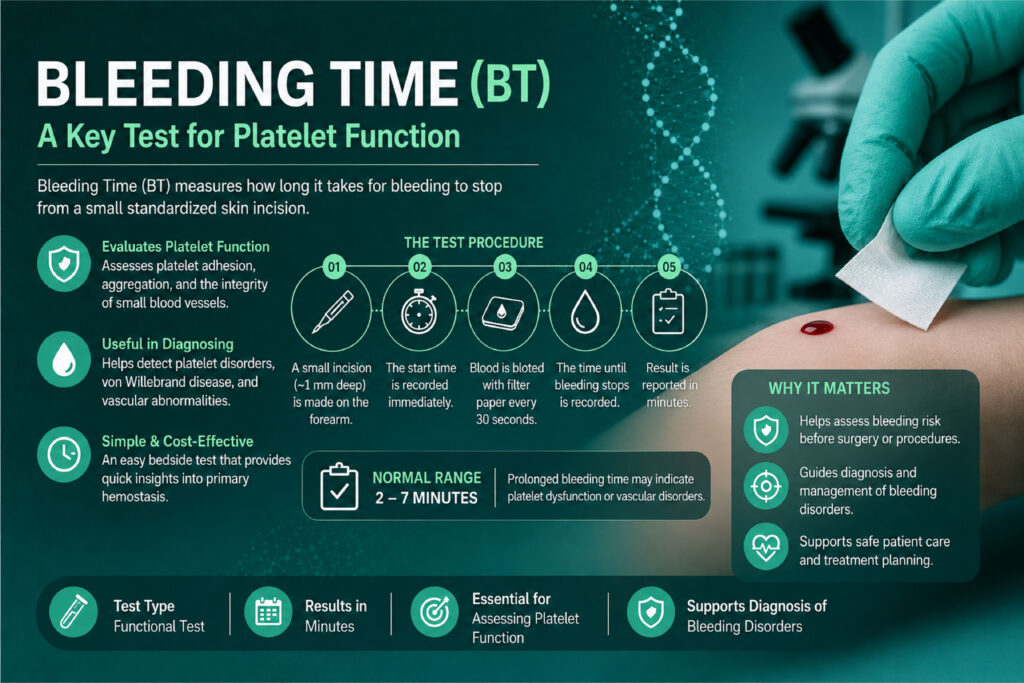
Table of Contents
Definition
The bleeding time test is an in vivo diagnostic assay that measures the time it takes for a small, standardized superficial skin incision to stop bleeding. It directly evaluates the efficiency of primary hemostasis—the immediate cellular response to vascular injury.
Vascular Injury ➔ Endothelial Exposure ➔ Platelet Adhesion (vWF) ➔ Platelet Activation & Aggregation ➔ Primary Platelet PlugClinical Significance
When interpreting a prolonged bleeding time, the clinical diagnostic framework must be categorized into four distinct pathophysiological areas: quantitative platelet defects, qualitative (functional) platelet defects, vascular wall disorders, and extrinsic/pharmacological interferences.
1. Quantitative Platelet Defects (Thrombocytopenia)
A decrease in the absolute number of circulating platelets is the most common cause of a prolonged bleeding time. Without an adequate mass of platelets, the formation of the primary platelet plug is physically delayed.
The Clinical Threshold: Generally, the bleeding time remains unaffected until the platelet count drops below 100,000/µL. However, it becomes linearly and significantly prolonged as the count falls below 50,000/µL. If a patient’s platelet count is under 20,000/µL, performing a bleeding time test is clinically contraindicated, as it poses an unnecessary risk of persistent hemorrhage.
Key Etiologies:
Bone Marrow Suppression: Reduced production due to aplastic anemia, leukemia, chemotherapy, or radiotherapy.
Increased Destruction: Immune Thrombotic Thrombocytopenic Purpura (ITP) or Disseminated Intravascular Coagulation (DIC), where consumption overrides production.
Splenic Sequestration: Hypersplenism trapping a massive fraction of the body’s platelets.
2. Qualitative Platelet Defects (Functional Inherited Disorders)
When a patient presents with a normal platelet count but a prolonged bleeding time, the clinical focus immediately shifts to functional anomalies. These are categorized by the specific stage of primary hemostasis that fails.
A. Adhesion Defects (The Anchor Fails)
Before platelets can aggregate, they must anchor to the exposed subendothelium. This requires von Willebrand Factor (vWF) acting as a bridge between subendothelial collagen and the platelet surface receptor Glycoprotein Ib/IX/V (GPIb/IX/V).
von Willebrand Disease (vWD): This is the most common inherited bleeding disorder worldwide. Whether it is a quantitative deficiency (Type 1 and Type 3) or a qualitative defect (Type 2) of vWF, the lack of functional bridge proteins causes a marked prolongation of bleeding time.
Bernard-Soulier Syndrome (BSS): A rare, autosomal recessive disorder characterized by a deficiency or mutation in the GPIb/IX/V receptor complex. In the lab, BSS presents with a prolonged bleeding time, mild-to-moderate thrombocytopenia, and uniquely giant platelets on a peripheral blood smear.
B. Aggregation Defects (The Bridge Fails)
Once platelets adhere and become activated, they express the surface receptor Glycoprotein IIb/IIIa (GPIIb/IIIa). This receptor binds to plasma fibrinogen, linking individual platelets together into a cohesive plug.
Glanzmann Thrombasthenia (GT): An autosomal recessive disorder caused by a severe deficiency or absence of the GPIIb/IIIa complex. Because platelets cannot cross-link via fibrinogen, aggregation is entirely absent. Patients present with a normal platelet count, normal platelet morphology, but an indefinitely prolonged bleeding time and severe mucosal bleeding.
C. Platelet Secretion/Granule Defects (The Signal Fails)
Activated platelets must release the contents of their dense granules (ADP, ATP, calcium, serotonin) and alpha granules (vWF, fibrinogen, Factor V) to recruit and activate neighboring platelets.
Storage Pool Diseases: Conditions like Hermansky-Pudlak syndrome or Chédiak-Higashi syndrome involve a deficiency in dense granules.
Gray Platelet Syndrome: A rare deficiency in alpha-granules, giving platelets a characteristically ghost-like, gray appearance on a Wright-stained blood smear. Both granule disorders yield a mildly to moderately prolonged bleeding time due to poor amplification of the clotting response.
3. Acquired and Drug-Induced Platelet Dysfunctions
In an acute clinical setting, acquired causes of functional platelet defects are far more prevalent than inherited disorders.
Irreversible COX-1 Inhibition (Aspirin): Acetylsalicylic acid permanently acetylates the cyclooxygenase-1 (COX-1) enzyme within platelets. This completely blocks the conversion of arachidonic acid into Thromboxane A_2 (TXA_2), a potent platelet agonist and vasoconstrictor. Because platelets lack a nucleus, they cannot synthesize new enzymes; thus, a single dose of aspirin disrupts platelet function—and prolongs bleeding time—for the entire 7-to-10-day lifespan of those circulating platelets.
Reversible COX Inhibition (NSAIDs): Medications like ibuprofen and naproxen temporarily block COX-1. Bleeding time normalizes once the drug clears from circulation (typically within 24–48 hours).
Uremia (Chronic Kidney Disease): In patients with advanced renal failure, a buildup of circulating uremic toxins (such as guanidinosuccinic acid) severely disrupts both platelet-to-endothelium adhesion and subsequent platelet aggregation. Managing these patients requires monitoring via bleeding time or automated PFA assays prior to invasive surgical procedures.
4. Vascular Wall Disorders (Endothelial / Tissue Defects)
In rare clinical scenarios, a patient may possess perfectly normal platelet counts and completely functional platelets, yet exhibit a prolonged bleeding time. This points to structural or connective tissue failures within the blood vessel wall itself, which prevents normal vasoconstriction and support for the platelet plug.
Scurvy (Vitamin C Deficiency): Vitamin C is a mandatory cofactor for collagen synthesis. Defective collagen weakens the perivascular supportive tissue, causing capillaries to rupture easily and fail to anchor platelets efficiently.
Ehlers-Danlos & Marfan Syndromes: Inherited connective tissue disorders that alter systemic collagen and elastic fibers, yielding fragile microvasculature and prolonged bleeding times.
Senile Purpura: Age-related degradation of dermal collagen and subcutaneous fat, leaving superficial blood vessels unprotected against minimal shear force.
Summary Diagnostic Matrix for Coagulation Profiles
To help differentiate where a prolonged Bleeding Time fits into a wider clinical workup, consider how it interacts with secondary hemostasis testing (PT and APTT):
| Clinical Condition | Bleeding Time (BT) | Platelet Count | Prothrombin Time (PT) | Activated Partial Thromboplastin Time (APTT) |
| Aspirin / NSAID Use | Prolonged | Normal | Normal | Normal |
| von Willebrand Disease | Prolonged | Normal (usually) | Normal | Prolonged (due to concurrent Factor VIII deficiency) |
| Glanzmann Thrombasthenia | Prolonged | Normal | Normal | Normal |
| Bernard-Soulier Syndrome | Prolonged | Decreased (Mild) | Normal | Normal |
| Immune Thrombocytopenia (ITP) | Prolonged | Decreased | Normal | Normal |
| Hemophilia A or B | Normal | Normal | Normal | Prolonged |
| Vitamin K Deficiency / Warfarin | Normal | Normal | Prolonged | Prolonged (in severe cases) |
Methods and Principle
1. The Core Principle of Bleeding Time
The fundamental principle of the bleeding time (BT) test is to measure the duration required for primary hemostasis to stop bleeding following a standardized, superficial incision of the microvasculature.
When an incision is made, the assay monitors three interdependent physiological mechanisms operating in real time:
Vascular Response (Vasoconstriction): Immediate local reflex vasoconstriction occurs to reduce local blood flow and pressure at the injury site.
Platelet Adhesion: Exposed subendothelial collagen binds to circulating von Willebrand Factor (vWF), which simultaneously captures passing platelets via their surface Glycoprotein Ib/IX/V (GPIb/IX/V) receptor complexes.
Platelet Activation and Aggregation: Attached platelets undergo structural transformation (shape change) and discharge their alpha and dense granules. Released adenosine diphosphate (ADP) and Thromboxane A_2 (TXA_2) recruit additional platelets. These cross-link with one another via plasma fibrinogen binding to activated Glycoprotein IIb/IIIa (GPIIb/IIIa) receptors, completing the primary platelet plug.
Because the shedding blood is blotted away without touching the wound bed, the endpoint—the definitive cessation of bleeding—signals that a stable, impermeable primary platelet plug has completely sealed the severed capillaries.
2. Step-by-Step Methodologies
To achieve clinical accuracy, manual bleeding time techniques require strict adherence to standardized parameters to minimize variables like depth, pressure, and touch-induced plug disruption.
A. The Ivy Method (The Template Standard)
The Ivy technique (and its modern commercial modification, the Template Method) is the clinical gold standard for manual testing due to its control over tissue tension and capillary hydrostatic pressure.
Materials Required
Sphygmomanometer (Blood pressure cuff)
Standardged automated template incision device (e.g., Simplate or Surgicutt), pre-calibrated to deliver an incision 5 mm long and 1 mm deep
Whatman No. 1 circular filter paper (or equivalent absorbent blotting paper)
Stopwatch / Timer
70% Isopropyl alcohol swabs and sterile adhesive bandage
Procedural Sequence
1.Patient Positioning and Site Selection:Prep Phase.
Extend the patient’s arm and support it firmly on a flat surface. Select an area on the volar (under) surface of the forearm, approximately three finger-widths below the antecubital fossa. Meticulously avoid visible superficial veins, scars, hair, or skin blemishes. Cleanse the site with 70% alcohol and allow it to air-dry completely to prevent chemical hemolysis or stinging.
2.Apply and Maintain Hydrostatic Pressure:Pressure Standardization.
Place the blood pressure cuff on the upper arm. Inflate the cuff precisely to 40 mmHg. This pressure must be held completely constant throughout the entirety of the procedure to distend the capillaries uniformly. Start the incision within 30 to 60 seconds of inflation.
3.Perform the Standardized Incision:Incision Phase.
Hold the patient’s forearm skin taut from behind the arm to create a uniform, flat landing zone. Press the automated template blade device firmly against the skin parallel to the length of the arm (longitudinal incision). Depress the trigger to fire the spring-loaded blade and start the stopwatch simultaneously. Discard the single-use device immediately into a sharps container.
4.Meticulous Blotting Technique:Every 30 Seconds.
As blood pools, bring the clean edge of the filter paper close to the wound every 30 seconds. Allow the drop of blood to wick onto the paper via capillary action. Crucial Safety Rule: Do not let the filter paper touch the raw edges of the skin incision itself. Touching the wound can physically dislodge the microscopic platelet plug and cause an artificially prolonged result.
5.Determine Endpoint and Post-Op Care:Completion Phase.
Repeat the blotting sequence every 30 seconds. The moment the filter paper no longer absorbs red blood, stop the timer. Record the elapsed time to the nearest half-minute. Deflate and remove the blood pressure cuff immediately. Apply a butterfly or standard adhesive bandage firmly over the site, instructing the patient to keep it in place for 24 hours to minimize minor scarring.
Normal Ivy Reference Range: 2.0 to 9.0 minutes (120 to 540 seconds).
B. The Duke Method (Historical Approach)
The Duke method is an older technique that lacks pressure standardization. While largely obsolete in modern diagnostic clinical laboratories, it serves as an alternative point-of-care method in resource-limited field clinics.
Materials Required
Sterile, standard single-use blood lancet (typically 2 mm depth)
Whatman No. 1 filter paper
Stopwatch
Alcohol swabs
Procedural Sequence
Site Selection: Cleanse the lower edge of the patient’s earlobe (or occasionally a digital fingertip) with alcohol. Allow it to air-dry completely.
Puncture: Perform a quick, firm puncture using the sterile lancet. The puncture should be deep enough to ensure spontaneous blood flow without needing to squeeze or “milk” the tissue (milking introduces tissue juices/thromboplastin, which activates clotting prematurely). Start the stopwatch immediately.
Blotting: Every 30 seconds, gently bring the filter paper into contact with the escaping droplet of blood, avoiding direct skin contact.
Endpoint: Stop the timer the exact moment blood stops staining the paper.
Normal Duke Reference Range: 1.0 to 3.0 minutes (60 to 180 seconds).
3. Methodological Comparison: Ivy vs. Duke
| Technical Parameter | Ivy (Template) Method | Duke Method |
| Primary Testing Site | Volar aspect of the forearm | Earlobe or fingertip |
| Standardized Pressure | Yes (Constant 40 mmHg via cuff) | No (Subject to atmospheric/tissue pressure) |
| Incision Control | Automated mechanical blade (Uniform 5mm x 1mm) | Manual lancet puncture (Highly variable depth) |
| Sensitivity to Defects | High (Highly sensitive to vWD and mild platelet disorders) | Low (Only detects severe hemostatic defects) |
| Risk of Complications | Minimal risk of minor keloid/scarring | Risk of hematoma, pain, or prolonged un-cuffed bleeding |
4. Troubleshooting Pre-Analytical Variables
The bleeding time test is notoriously sensitive to technical variations. To maintain technical quality control, look out for these specific pre-analytical confounders:
Residual Alcohol: If the cleansing alcohol does not fully dry, it dilutes the escaping blood, impairs native local vasoconstriction, and causes localized lysis of red blood cells.
Improper Cuff Tension: If the blood pressure cuff drops below 40 mmHg, it reduces the pressure head inside the microvasculature, leading to a falsely shortened bleeding time. If it exceeds 40 mmHg, it can overwhelm the emerging platelet plug, causing false prolongation or hematoma.
Hematoma Formation: If an incision is accidentally made directly over a larger superficial vein, blood will pool rapidly under the skin or cascade from the wound, invalidating the test. The procedure must be aborted and restarted on the alternate arm.
Specimen Requirements
Because the Bleeding Time (BT) test is an in vivo functional assay, its specimen requirements differ fundamentally from almost every other test in the clinical laboratory. There is no test tube, no anticoagulant selection, and no centrifugation phase.
The specimen is the patient’s living, intact microvasculature.
Because the sample cannot be preserved, stored, or re-run, strict adherence to patient preparation, physiological screening, and site criteria constitutes the entire “specimen collection” protocol.
1. Pre-Analytical Patient Screening & Physiological Requirements
Before bringing a blade to a patient’s skin, you must verify that their physiology has not been altered by external biochemical factors. Pre-analytical interference is the leading cause of false-positive (artificially prolonged) bleeding times.
The Antiplatelet Exclusion Window
You must screen the patient for the ingestion of any substances that inhibit platelet function. If any of the following have been consumed, the laboratory must document it and consult the ordering physician before proceeding:
Irreversible Inhibitors (7-Day Deferral): Aspirin (acetylsalicylic acid) and aspirin-containing compound medications (e.g., certain cold remedies or migraine formulations) must be discontinued for a full 7 days prior to the test. This duration matches the standard lifespan of a circulating platelet.
Reversible Inhibitors (48-Hour Deferral): Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) such as ibuprofen, naproxen, indomethacin, and diclofenac must be avoided for at least 48 hours.
Dietary & Herbal Agents (48-Hour Deferral): High doses of Vitamin E, garlic supplements, ginkgo biloba, ginger, and ginseng can alter platelet membrane dynamics and should be paused for 48 hours.
Recent Alcohol Consumption: Alcohol suppresses thromboxane A_2 synthesis transiently. Patients should abstain from alcohol for 24 hours before the procedure.
Baseline Platelet Count Verification
Before performing an invasive bleeding time test, a recent Complete Blood Count (CBC) should be reviewed.
The baseline platelet count should ideally be greater than 50,000/µL.
If a patient has severe thrombocytopenia (under 50,000/µL), the bleeding time is virtually guaranteed to be prolonged. Running the test provides no added diagnostic value regarding platelet function and subjects the patient to an unnecessary risk of persistent bleeding or hematoma.
2. Anatomical Specimen Site Requirements
The anatomical site chosen for the incision must meet precise physical criteria to ensure that the blood flowing from the microvasculature reflects true primary hemostasis, free from confounding tissue variables.
Ideal Site: Volar Forearm ➔ 3 Finger-Widths Below Antecubital Fossa ➔ Free of Veins, Scars, and Hair
For the Ivy / Template Method
Primary Location: The volar (inner) surface of the forearm.
Zonal Boundaries: Approximately 3 to 5 cm (about three finger-widths) below the antecubital fossa (the crease of the elbow).
Tissue Criteria:
No Superficial Veins: The site must be carefully inspected under bright light. Incising a visible superficial vein will introduce high venous pressure, causing rapid, heavy bleeding that overwhelms the forming platelet plug and invalidates the test.
No Scars or Keloids: Fibrotic scar tissue has altered vascularity and compromised collagen architecture, which prevents proper platelet adhesion via von Willebrand Factor.
No Edema or Lesions: Edematous tissue contains excess interstitial fluid that dilutes the escaping blood and alters local tissue turgor pressure. Avoid areas with rashes, infections, or tattoos.
Minimal Hair: Excessive hair can trap blood droplets, making clean wicking onto filter paper impossible. If necessary, a site with minimal hair should be selected; shaving is discouraged immediately before the test as it can cause micro-abrasions that trigger localized clotting.
For the Duke Method (Historical/Alternative)
Primary Location: The fleshy, inferior margin of the earlobe or, alternatively, the lateral aspect of a digital fingertip.
Tissue Criteria: The site must be warm and well-perfused. It must be completely free of cold-induced vasoconstriction, piercings, active skin infections, or cyanosis.
3. Environmental and Physiological Homeostasis
Because the specimen is a living vascular bed, it reacts instantly to external physical stimuli. The collection environment must be strictly controlled:
Temperature Stability: The testing room must be kept at a comfortable ambient temperature (20°C to 25°C). Cold environments cause systemic reflex vasoconstriction, which can artificially shorten the bleeding time. Excessive heat causes vasodilation, which can prolong it. If the patient’s arm feels cold to the touch, warm it gently with a warm towel prior to disinfection.
Patient State: The patient should be calm and seated or reclining comfortably for at least 10 minutes prior to the test. High anxiety or physical exertion spikes blood pressure and circulating epinephrine, altering native vascular tone and capillary dynamics.
Summary Checklist for BT Specimen Acceptance
| Parameter | Mandatory Requirement | Action if Requirement Fails |
| Aspirin / Antiplatelet Intake | None within the last 7 days | Contact physician; usually requires rescheduling. |
| NSAID Intake | None within the last 48 hours | Note on chart or defer test by 2 days. |
| Platelet Count Baseline | Greater than 50,000/µL | Defer test; bleeding time will be prolonged due to low mass alone. |
| Anatomical Site Selection | Volar forearm; zero superficial veins or scars | Shift site laterally or use the alternate arm. |
| Skin Temperature | Warm to the touch; normal perfusion | Apply a warm compress before beginning site prep. |
Reference Ranges and Clinical Interpretations
1. Reference Ranges
Because Bleeding Time (BT) is a manual, non-automated test, reference intervals can vary slightly based on the specific commercial device used (such as Simplate or Surgicutt) and local laboratory validation studies. However, standard clinical practice accepts the following definitive ranges:
| Method | Normal Reference Range | Borderline / Equivocal Zone | Prolonged (Abnormal) Threshold | Critical Value / Panic Limit |
| Ivy / Template Method | 2.0 to 9.0 minutes (120 – 540 seconds) | 9.1 to 10.0 minutes | Greater than 10.0 minutes | Greater than 15.0 minutes |
| Duke Method | 1.0 to 3.0 minutes (60 – 180 seconds) | 3.1 to 4.0 minutes | Greater than 4.0 minutes | Greater than 8.0 minutes |
Key Reference Ranges
The Equivocal Zone: A result between 9 and 10 minutes (Ivy) is considered borderline. It requires a thorough chart review for hidden pre-analytical variables (like a missed low-dose aspirin or NSAID) and should generally be repeated on the opposite arm or followed up with an automated Platelet Function Analysis (PFA-100).
The Critical Value Alert: A bleeding time exceeding 15 minutes using the Ivy method represents a critical value. The testing technologist must immediately stop blotting, apply firm, direct pressure to the wound with sterile gauze to prevent hematoma or severe blood loss, bandage the site securely, and notify the ordering clinician immediately.
2. Advanced Clinical Interpretations: Diagnostic Decision Tree
Interpreting an abnormal bleeding time requires evaluating it alongside a full Coagulation Profile—specifically the Platelet Count, Prothrombin Time (PT), and Activated Partial Thromboplastin Time (APTT).
A isolated prolonged bleeding time points directly to a defect in primary hemostasis (platelets or vessel walls), whereas abnormalities in PT or APTT point to secondary hemostasis (clotting factors).
[ PROLONGED BLEEDING TIME ]
│
Check Baseline Platelet Count
│
┌───────────────────┴───────────────────┐
▼ ▼
[ Decreased (<50k/µL) ] [ Normal Platelet Count ]
│ │
Quantitative Defect Evaluate PT & APTT
(Thrombocytopenia) │
┌──────────────┴──────────────┐
▼ ▼
[ PT & APTT Normal ] [ APTT Prolonged, PT Normal ]
│ │
Qualitative Defect Possible von Willebrand
(Drugs, GT, BSS, Vascular) Disease (vWD) Type 1/2
Scenario A: Prolonged BT with a Decreased Platelet Count
This points directly to a Quantitative Platelet Defect (Thrombocytopenia). The prolongation is due to a lack of platelet mass rather than a functional issue.
Clinical Diagnostic Path: Investigate bone marrow production (aplastic anemia, leukemia) or accelerated peripheral destruction/consumption (Immune Thrombocytopenic Purpura [ITP], Thrombotic Thrombocytopenic Purpura [TTP], or early Disseminated Intravascular Coagulation [DIC]).
Scenario B: Prolonged BT with a Normal Platelet Count and Normal PT / APTT
This indicates a Qualitative (Functional) Platelet Defect or a Vascular Wall Disorder. The platelets are present in adequate numbers, but they cannot function, or the vessels cannot constrict.
Drug-Induced Dysfunction: Irreversible inhibition of cyclooxygenase-1 (COX-1) by Aspirin, or reversible inhibition by NSAIDs (ibuprofen).
Glanzmann Thrombasthenia: Rare inherited absence of the GPIIb/IIIa receptor, which completely blocks platelet-to-platelet aggregation.
Uremic Platelet Dysfunction: Chronic Kidney Disease (CKD) toxins coat the platelet membranes, impairing adhesion and aggregation.
Vascular Fragility: Connective tissue diseases like Scurvy (Vitamin C deficiency) or Ehlers-Danlos Syndrome, where abnormal collagen prevents vessels from supporting plug formation.
Scenario C: Prolonged BT with a Normal Platelet Count and a Prolonged APTT
This classic combination narrows the diagnosis down to two major primary hemostatic pathways:
von Willebrand Disease (vWD): Because von Willebrand Factor (vWF) acts as the essential “anchor” for platelet adhesion and serves as the stabilizing carrier protein for Factor VIII in plasma, a deficiency in vWF causes both a prolonged bleeding time (adhesion failure) and a prolonged APTT (Factor VIII deficiency).
Bernard-Soulier Syndrome: An inherited deficiency of the GPIb/IX/V receptor complex. It presents with a prolonged bleeding time, normal PT/APTT, and characteristically giant platelets on a peripheral blood film, often accompanied by mild thrombocytopenia.
3. Causes of an Artificially Shortened Bleeding Time
While a prolonged result takes center stage clinically, an unexpectedly short bleeding time (e.g., less than 1.5 minutes via Ivy) can also occur and is almost always driven by technical or physiological anomalies:
Elevated Hematocrit (Polycythemia): A high red blood cell mass pushes platelets laterally toward the endothelial wall of the blood vessels (a phenomenon known as marginalization). This high concentration speeds up adhesion and can cause an artificially shortened bleeding time.
Pre-Analytical Technical Errors:
Inflating the blood pressure cuff below 40 mmHg reduces venous backpressure, allowing the wound to seal too rapidly.
Making an insufficient or shallow incision (less than 1 mm deep) that fails to sever the capillary bed adequately.
Accidental direct contact with the wound using the filter paper, which can pack the emerging platelets together mechanically and stop blood flow prematurely.
4. Differential Diagnosis Laboratory Matrix
To systematically rule out confounding disorders when evaluating abnormal BT results, reference this comprehensive diagnostic framework:
| Suspected Clinical Condition | Bleeding Time (BT) | Platelet Count | PT | APTT | Platelet Aggregometry Studies |
| Aspirin Therapy | Prolonged | Normal | Normal | Normal | Normal response to Ristocetin; Decreased response to Arachidonic Acid |
| von Willebrand Disease | Prolonged | Normal | Normal | Prolonged | Abnormal response to Ristocetin; Normal response to ADP/Collagen |
| Glanzmann Thrombasthenia | Prolonged | Normal | Normal | Normal | Normal response to Ristocetin; Absent response to ADP, Collagen, Epinephrine |
| Bernard-Soulier Syndrome | Prolonged | Decreased | Normal | Normal | Absent response to Ristocetin; Uncorrected by adding normal plasma |
| Uremia (Advanced CKD) | Prolonged | Normal | Normal | Normal | Variable/multi-receptor down-regulation |
| Hemophilia A (Factor VIII) | Normal | Normal | Normal | Prolonged | Completely Normal |
Quick Stats
| Feature | Details | Critical Lab Insights |
| Test Type | Coagulation / Functional Hemostasis Marker | A direct in vivo indicator of primary hemostasis. It uniquely evaluates the functional interaction between platelets and the vascular endothelium under active pressure. |
| Sample Type | Living, Intact Microvasculature (In Vivo) | No test tube, anticoagulant, or centrifugation phase exists. The specimen is the patient’s circulating capillary bed, making the test non-storable and non-repeatable. |
| Method Standard | Ivy (Template) Method | The clinical standard. It uses a blood pressure cuff inflated to 40 mmHg to standardize capillary hydrostatic pressure and an automated device for uniform incision dimensions. |
| Primary Metric | Elapsed Time (Minutes and Seconds) | Measured from the exact second of the incision to the complete cessation of macrovascular bleeding onto filter paper. |
| Patient Prep Window | 7-Day Antiplatelet Exclusion | Irreversible platelet inhibitors (Aspirin) must be ceased for 7 days (the lifetime of a platelet). Reversible inhibitors (NSAIDs) require a 48-hour deferral to avoid false prolongation. |
| Baseline Requirement | Platelet Count > 50,000/µL | A baseline CBC must be checked. If a patient has severe thrombocytopenia, the BT will be prolonged due to low platelet mass alone, destroying its utility as a functional assay. |
| Testing Interval | 30-Second Blotting Cadence | Blood must be wicked onto filter paper precisely every 30 seconds. Crucial: The paper must never touch the skin or incision directly, as this dislodges the developing platelet plug. |
| Normal Reference Range | 2.0 – 9.0 Minutes (Ivy Method) | Device-dependent. Borderline ranges (9.1–10.0 mins) warrant clinical chart correlation, while the historical Duke method (earlobe) ranges much shorter at 1.0–3.0 minutes. |
| Critical Panic Value | > 15.0 Minutes (Ivy Method) | If bleeding exceeds 15 minutes, the technologist must abort the test, apply immediate, firm direct pressure with sterile gauze to prevent hematoma, and notify the clinician. |
| Key Limitation | High Pre-Analytical Variability | Highly operator-dependent. Results are easily skewed by poor cuff pressure maintenance, improper anatomical site selection (e.g., over a superficial vein), or direct wound contact. |
FAQs
1. Why does von Willebrand Disease (vWD) prolong both Bleeding Time and APTT, while Hemophilia only prolongs APTT?
This is a classic board exam question that tests your understanding of primary versus secondary hemostasis.
Bleeding Time evaluates primary hemostasis. von Willebrand Factor (vWF) is the mandatory “anchor” that binds platelets to subendothelial collagen. Without it, platelets cannot adhere, resulting in a prolonged BT.
APTT evaluates the intrinsic and common pathways of secondary hemostasis. In plasma, vWF acts as a protective carrier protein that stabilizes Factor VIII. Without vWF, Factor VIII is rapidly degraded, leading to a prolonged APTT.
In Hemophilia (A or B), the defect lies strictly within the clotting factors (Factor VIII or IX) of secondary hemostasis. Platelet number, platelet function, and vWF levels are completely normal, which is why hemophiliacs present with a perfectly normal Bleeding Time.
2. What happens to the Bleeding Time if a patient takes a single dose of Aspirin versus a dose of Ibuprofen?
Both drugs inhibit the cyclooxygenase (COX) pathway, but their mechanisms differ fundamentally in duration:
Aspirin is an irreversible inhibitor. It permanently acetylates the COX-1 enzyme, completely blocking the production of Thromboxane A_2 (TXA_2) for the entire lifespan of that platelet (~7 to 10 days). Because platelets lack a nucleus, they cannot synthesize new enzymes. Therefore, a single aspirin can prolong BT for up to a week.
Ibuprofen (and most NSAIDs) is a reversible inhibitor. It binds temporarily to the COX-1 enzyme. Once the drug is cleared from the plasma (usually within 24 to 48 hours), the platelets regain their normal functional capacity, and the Bleeding Time returns to the baseline reference range.
3. If a patient’s Bleeding Time exceeds 15 minutes during an Ivy test, what is the exact laboratory protocol?
A result exceeding 15 minutes is considered a Critical/Panic Value for manual hemostasis testing. The testing technologist must execute the following safety protocol:
Abort the test: Stop timing and immediately stop blotting the wound.
Apply Direct Mechanical Pressure: Place a sterile gauze pad over the incision and apply firm, continuous direct pressure.
Deflate the Cuff: Immediately release the blood pressure cuff to remove the 40 mmHg hydrostatic pressure head from the capillaries.
Secure the Wound: Maintain pressure until the bleeding stops completely, then apply a tight butterfly bandage or sterile pressure dressing.
Report the Critical Value: Document the exact time the test was stopped (e.g., “>15 minutes”) and immediately phone the ordering physician or ward nurse to report the critical bleeding risk.
4. Why is the Ivy method clinically superior to the historical Duke method?
The Ivy method (and its modern automated template variants) significantly reduces pre-analytical operator error through two key standardizations:
Hydrostatic Pressure Control: By using a blood pressure cuff inflated strictly to 40 mmHg, the Ivy method ensures that the capillary beds are under uniform, reproducible pressure across all patients. The Duke method (earlobe puncture) relies entirely on native, un-standardized tissue pressure.
Incision Consistency: The Ivy method uses a standardized, spring-loaded mechanical blade that ensures the incision is precisely 5 mm long and 1 mm deep. The Duke method relies on a manual lancet puncture, which varies drastically in depth depending on how hard the technologist presses.
5. Can a patient with a normal platelet count have a prolonged Bleeding Time?
Yes. This presentation is the exact clinical indication for performing a functional platelet assay. If the platelet count is normal (e.g., 250,000/µL) but the Bleeding Time is prolonged, the patient has a qualitative platelet defect or a vascular wall disorder.
The laboratory should immediately follow up with a chart review for antiplatelet medications (Aspirin) or order advanced testing, such as Platelet Aggregometry to rule out inherited receptor deficiencies like Glanzmann Thrombasthenia (GPIIb/IIIa defect) or Bernard-Soulier Syndrome (GPIb/IX/V defect).